

European Journal of Neurodegenerative Diseases 2023; 12(1) January-April 20-23
OLFACTORY DYSFUNCTION AS A PREDICTOR OF THE FUTURE DEVELOPMENT OF PARKINSONISM IN COVID-19 PATIENTS: A 18F-FDOPA PET STUDY
M.A. De Rosa1+, D. Calisi1+, C. Carrarini1, A. Mazzatenta1, M.V. Mattoli2, G. Neri1, D. D’Ardes3, R. Giansante4, M. Onofrj1, L. Stuppia4, F. Cipollone3, L. Bonanni3*
1 Department of Neuroscience, Imaging and Clinical Sciences, G. D’Annunzio University of Chieti-Pescara, Chieti, Italy
2 Department of Nuclear Medicine Unit, Presidio Ospedaliero Santo Spirito, Pescara, Italy
3 Department of Medicine and Aging Sciences, G. D’Annunzio University of Chieti-Pescara, Chieti, Italy
4 Department of Psychological, Health and Territory Sciences, School of Medicine and Health Sciences, G. D’Annunzio University of Chieti-Pescara, Chieti, Italy
+These authors contributed to this study
*Correspondence to:
Laura Bonanni, MD, PhD,
Department of Medicine and Aging Sciences,
D’Annunzio University of Chieti-Pescara,
Chieti, Italy
e-mail: l.bonanni@unich.it
Received: 02 March2023 Accepted: 05 April 2023 |
2974-6345 (2023) Copyright © by BIOLIFE |
ABSTRACT
Background: Among the various clinical manifestations of COVID-19, olfactory dysfunction is reported in 68% of patients, and is persistent in 10%. When inhaled, the virus travels along the olfactory pathway, infects the olfactory bulb and can retrogradely attack, through a direct nigro-olfactory connection, the Substantia Nigra. The evidence of cases of parkinsonism after SARS-CoV-2 infection that are preceded by olfactory dysfunction highlights a possible link between SARS-CoV-2 infection and the subsequent development of parkinsonism. Here, we report two cases out of 4 patients with long-term olfactory dysfunction, persistent at 4-9 months after SARS- CoV-2 infection, who presented with dopaminergic imaging abnormalities. Methods: The patients underwent nasal endoscopy, olfactory smart threshold test, and olfactory event-related potentials, were examined by movement disorder specialists for parkinsonian signs (with UPDRS part III), and underwent positron emission tomography (PET) imaging with 3,4-Dihydroxy-6-(18F)fluoro-L-phenylalanine (18F-FDOPA). Results: Nasal endoscopy was normal. Both patients resulted anosmic at both the olfactory smart threshold test and the olfactory event-related potentials, and showed a minimal reduction in tracer concentration in the posterior portion of the putamen bilaterally in absence of clinical parkinsonism. Conclusion: 18F-FDOPA PET showed damage to the basal ganglia in patients with persistent olfactory dysfunction after SARS-Cov2 infection, highlighting the presence of an olfactory-nigral dysfunction, possibly representing a pre-clinical signature of parkinsonism. Follow-up and longitudinal studies should verify this hypothesis.
KEYWORDS: SARS-CoV-2, COVID, parkinsonism, olfactory dysfunction, 18F-FDOPA, olfactory-nigral pathway
INTRODUCTION
Among the various clinical manifestations of SARS-CoV-2 disease (COVID-19), olfactory dysfunction (OD) is reported in 68% of patients and results are persistent in 10%. OD can depend on the neuroinvasive properties of the virus, which could reach the olfactory bulb (OB) through the olfactory mucosa and neurons (1). SARS-CoV-2 also induces an inflammatory response in the Central Nervous System (CNS) that can reduce the sense of smell. SARS-CoV-2 shares characteristics with the influenza virus H1N1, that was responsible for the 1918 Spanish flu outbreak, and the subsequent Encephalitis Lethargica (EL), which was followed by an increased incidence of post-encephalitic parkinsonism (2, 3). Destruction of the Substantia Nigra (SN), responsible for the pathogenesis of parkinsonism, was demonstrated in EL. The etiology of post-encephalitic parkinsonism has been recently linked to the olfactory vector hypothesis (2). When inhaled, the virus travels along the olfactory pathway and infects the OB to attack the SN (1) retrogradely. Degeneration of this nigro-olfactory connection may be involved in parkinsonism, where hyposmia is a prodromal symptom. Other Coronaviruses have been demonstrated to cause CNS neuronal death through the nasal cavity, and basal ganglia lesions have been discovered related to thromboembolic encephalopathies (4). Additionally, a case of acute parkinsonism associated with COVID-19 infection has been previously reported (5). The evidence of cases of parkinsonism after COVID-19, that are preceded by OD, highlights a possible link between SARS-CoV-2 infection and the subsequent development of parkinsonism. Here we report two cases of persistent OD due to SARS-CoV-2 infection that presented with dopaminergic imaging abnormalities.
MATERIALS AND METHODS
Four patients, healed from a previous SARS-CoV-2 infection, were recruited by the COVID-19 Unit of the SS Annunziata Hospital of Chieti. A detailed medical history was collected for all patients. Nasal endoscopy was performed to exclude nasal causes of anosmia. The patients were tested with an olfactory smart threshold test (OST), which is useful for fast preliminary screening of the olfactory function, that works based on four disposable items based on the Connecticut Chemosensory Clinical Research Center threshold test and the Italian population age phenotype threshold test (7).
Olfactory event-related potentials (OERPs) were also performed. OERPs consist of a negative component, the N1, followed by two positive components, P2 and P3. The early component (N1) reflects the exogenous cortical activity related to sensory input detection and primary sensory processing. In contrast, the later olfactory OERP components (P2 and P3) reflect endogenous cortical activity related to secondary cognitive processing (8). Latency (range of 530 to 800 ms after stimulus onset), amplitude (approximately between 4 and 20 μV), and shape are the main parameters of OERP components (8). OERPs are the results of a grand average of 10 stimulations recorded by EEG power lab equipment (AD-Instruments) following standard procedure, and are only detectable in the periphery at high concentrations (8, 9). The patients were subsequently examined by movement disorder specialists and clinical evaluations included a neurological examination with the Unified Parkinson’s Disease Rating Scale part III (UPDRS-III) (6).
Finally, patients underwent positron emission tomography (PET) imaging with 3,4-Dihydroxy-6-(18F) fluoro-L-phenylalanine, (18F-FDOPA). The patients, who fasted for at least 6 h, underwent an 18F-FDOPA brain scan using a PET-CT Discovery MI DR tomograph (GE Healthcare). PET-CT 15 minutes static image acquisition was performed 90 min after administration of 185MBq of 18F-FDOPA. No premedication with carbidopa was performed. A low-dose CT scan was performed for anatomical localization and for attenuation correction of PET images. PET-CT images were assessed qualitatively (10). Neurophysiological, clinical, and imaging assessments were conducted blindly for the results of all the tests.
RESULTS
The four patients (2 males, aged 55 and 62 years old, and 2 females, aged 49 and 75 years old) healed from COVID-19 without remarkable sequelae besides anosmia and had a normal nasal endoscopy. Anosmia was confirmed by OST and OERPs. Clinical evaluation resulted as substantially normal in all the patients (except for mild rigidity in the 75 year old patient, detailed in the case report). Among them, two patients showed abnormal uptake in the putamina at the 18F-FDOPA brain scan. Here we report these two cases.
Case 1
Patient 1 is a 49-year-old woman, with no relevant medical or pharmacological history. Her family history was negative for neurological diseases (i.e., parkinsonism). She was infected with SARS-CoV-2 during the first pandemic wave, in April 2020, without relevant respiratory symptoms. She was treated at home for flu-like symptoms, and she reported early anosmia and ageusia. She tested negative for SARS-CoV-2 at day 14 after the first positive swab, but OD persisted. Nasal endoscopy did not show nasal obstruction on the roof of the nasal fossa or turbinate hypertrophy. Anosmia was tested by the OST test (negative score to maximum concentration of n-butanol) and recognized as incomplete anosmia by OERPs (persistence of anomalous shape and duration trigeminal cross-modal perception, at 4 months after the acute disease) (Fig. 1a). Her neurological examination was normal; her UPDRS-III score was 0. A 18F-FDOPA-PET was performed to address the possible presence of olfactory-nigral involvement in the persistence of OD and showed minimal reduction in tracer concentration in the posterior portion of the putamen bilaterally (Fig. 1b).
Case 2
Patient 2 is a 75year old woman with hypertension with no history of neurological disorders. She had COVID-19 in May 2021 and was treated at home with corticosteroids and cholecalciferol for cephalalgia, sinusitis, and conjunctivitis. She had severe hyposmia. After recovery from the acute symptoms, OD persisted. Nasal endoscopy resulted normal. OD was confirmed by the OST test (negative score to a maximum concentration of n-butanol) and confirmed by OERPs performed at 9 months after the acute SARS-CoV-2 infection (Fig. 1c). She underwent neurological examination which was negative. Her UPDRS-III score was 6 due to mild rigidity of the neck and limbs. She underwent 18F-FDOPA-PET which showed a minimal reduction in tracer concentration in the posterior portion of the putamen bilaterally (Fig. 1d).
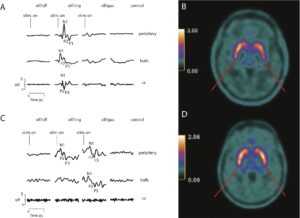

Fig. 1. A): Olfactory event-related potential (OERPs) of case 1: Electrophysiological recordings from the olfactory periphery, main olfactory bulb and vertex with unimodal olfactory stimulation (olf/olf, pure olfactory stimulation with orange odour, produced by citral) and cross-modal stimulations (olf/trig, olfactory/trigeminal with mint odour, produced by R-(-)-carvon and olf/gus olfactory/gustative with mushroom odour produced by n-octen-3-ol) compared to the unstimulated basal control recording. The patient shows OERP exclusively for the olfactory/trigeminal cross-modal stimulation, no signal is detectable for the other stimulations. The patient is to be considered “incomplete anosmic”. Trigeminal olfactory perception is however impaired because the signal is abnormal in shape, amplitude and duration; B): 18F-FDOPA-PET images of case 1 which show minimal reduction in tracer concentration in the posterior portion of the putamen bilaterally (red arrows); C): Olfactory event-related potential (OERPs) of case 2: Electrophysiological recordings from the olfactory periphery, main olfactory bulb and vertex with unimodal olfactory stimulation (olf/olf, pure olfactory stimulation with orange odour, produced by citral) and cross-modal stimulations (olf/trig, olfactory/trigeminal with mint odour, produced by R-(-)-carvon and olf/gus olfactory/gustative with mushroom odour produced by n-octen-3-ol) compared to the unstimulated basal control recording. The patient shows OERP in the olfactory periphery for cross-modal stimulations, of which only the olfactory/gustatory persists in the main olfactory bulb. In any case, no signal is detectable for any modalities in cz, so the patient is considered anosmic due to a deficit of the central electrophysiological signal; D): 18F-FDOPA-PET images of case 2 which show minimal reduction in tracer concentration in the posterior portion of the putamen bilaterally (red arrows).
DISCUSSION AND CONCLUSION
Our two patients with persistent OD after COVID presented with putaminal damage demonstrated by 18F-FDOPA-PET, likely due to an olfactory-nigral dysfunction caused by SARS-CoV2 infection. Even though the patients did not show clinical features of parkinsonism as assessed by UPDRS, they nevertheless showed the presence of putaminal involvement. This damage might be a prodromal sign of the possible future development of parkinsonism, as happened after the Spanish flu with the appearance of postencephalitic parkinsonism. The real epidemiological impact of such an association should be addressed by follow-up and longitudinal studies.
Statement of ethics
Written informed consent was obtained from the patients for publication of this case series and any accompanying images. The paper is exempt from ethical committee approval because it is not necessary for the publication of the case report. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding sources
Not applicable.
Data availability statement
Data is available from the corresponding author upon reasonable request.
REFERENCES
- R. Butowt, C.S. von Bartheld. Anosmia in COVID-19: Underlying Mechanisms and Assessment of an Olfactory Route to Brain Infection, Neurosci Rev J Bringing Neurobiol Neurol Psychiatry (2021) 27:582–603. https://doi.org/10.1177/1073858420956905
- I. Mori. Olfactory vector hypothesis for encephalitis lethargica, Med Hypotheses (2017) 103:128–130. https://doi.org/10.1016/j.mehy.2017.05.008
- R.T. Ravenholt, W.H. Foege. 1918 influenza, encephalitis lethargica, parkinsonism, Lancet Lond Engl (1982) 2:860–864. https://doi.org/10.1016/s0140-6736(82)90820-0
- D. Sulzer, A. Antonini, V. Leta, et al. COVID-19 and possible links with Parkinson’s disease and parkinsonism: from bench to bedside, NPJ Park Dis (2020) 6:18. https://doi.org/10.1038/s41531-020-00123-0
- A. Méndez-Guerrero, M.I. Laespada-García, A. Gómez-Grande, et al. Acute hypokinetic-rigid syndrome following SARS-CoV-2 infection, Neurology (2020) 95:e2109–e2118. https://doi.org/10.1212/WNL.0000000000010282
- C.G. Goetz, W.J. Weiner, P.A. Nausieda, H.L. Klawans, Tardive dyskinesia: pharmacology and clinical implications, Clin Neuropharmacol (1982) 5:3–22.
- A. Mazzatenta, A. Cellerino, N. Origlia, D. Barloscio, F. Sartucci, C. Di Giulio, L. Domenici. Olfactory phenotypic expression unveils human aging, Oncotarget (2016) 7:19193–19200. https://doi.org/10.18632/oncotarget.8393
- A. Mazzatenta, C. Montagnini, A. Brasacchio, F. Sartucci, G. Neri. Electrophysiological and olfactometric evaluation of long-term COVID-19, Physiol Rep (2021) 9:e14992. doi: 10.14814/phy2.14992
- S. Invitto, A. Mazzatenta. Olfactory Event-Related Potentials and Exhaled Organic Volatile Compounds: The Slow Link Between Olfactory Perception and Breath Metabolic Response. A Pilot Study on Phenylethyl Alcohol and Vaseline Oil, Brain Sci (2019) 9: 84. https://doi.org/10.3390/brainsci9040084
- S. Morbelli, G. Esposito, J.Arbizu, et al. Law, EANM practice guideline/SNMMI procedure standard for dopaminergic imaging in Parkinsonian syndromes 1.0., Eur J Nucl Med Mol Imaging (2020) 47:1885–1912. https://doi.org/10.1007/s00259-020-04817-8