

European Journal of Neurodegenerative Diseases 2017; 6(1) January-June: 6-9
IDEAL ASSIMILABLE AND BIOAVAILABLE PROTEIN COMPOUND: SUPPLEMENTARY DIETARY PROTEIN HELPS CANCER PATIENTS
M.L. Moretti
Director of the International Nutrition Research Center (INRC), Miami, USA.
*Correspondence to:
Maurizio Luca Moretti,
Director of the International Nutrition Research Center (INRC),
Miami, USA.
| Received: 09 January, 2017 Accepted: 01 April, 2017  |
2279-5855 (2017) Copyright © by BIOLIFE This publication and/or article is for individual use only and may not be further reproduced without written permission from the copyright holder. Unauthorized reproduction may result in financial and other penalties. Disclosure: all authors report no conflicts of interest relevant to this article. |
ABSTRACT
Proteins are the building blocks of organisms that are essential for carrying out daily cellular biological functions and for leading a healthy life. They are composed of a series of amino acids linked together, and have various metabolic defence functions for the organism. In some pathological states, such as cancer, anorexia, bulimia, dysmetabolism, malabsorption, vomiting, etc., there may be a protein deficiency. In subjects affected by cancer who are undergoing therapy, altered metabolism and progressive weight loss are common complications associated with protein deficiency. The loss of protein in tissues results from hepatic dysfunction which compromises the body’s ability to synthesize proteins. A high-protein compound containing essential amino acids, which is free of fat and sodium, could be indicated to compensate for protein deficiency, and can be useful for improving the quality of life for cancer patients.
Keywords: nutrition, protein, amino acid, metabolism, health
INTRODUCTION
Proteins are composed of amino acids and are the basic building blocks of organisms that serve many purposes for the human body. They have various metabolic defense functions for the organism and act as structural support, catalysts, enzymes, hormones, and initiators of cell death. Due to their many functions, proteins are vital for the daily biological functioning of cells and for maintaining proper health.
Protein deficiency may be present in some pathological conditions including cancer (1), anorexia and bulimia (2), malabsorption syndromes (3), dysmetabolism, and vomiting (4). Additionally, when various amino acids are transformed, proteins exert catabolic effects that can produce nitrogenous residues. For patients who have certain pathologies such as liver or kidney disease and neurological diseases, these nitrogenous residues are damaging (5,6). Furthermore, professional athletes may require an increased amount of protein due to the elevated demands of energy they are subjected to. For these reasons, a high-protein compound which includes essential amino acids, and that is free from fat and sodium, could be used in cases of protein deficiency.
DISCUSSION
Proteins are made up of the four fundamental elements carbon, hydrogen, oxygen, and nitrogen, and are composed of a set of amino acids linked by a peptide bond, forming chains that can be of varying lengths. Proteins are macromolecules (also called peptides) that are made up of chains of amino acids linked by an amine leg of an amino acid and a carboxyl group of another amino acid with the loss of a water molecule (Fig.1).
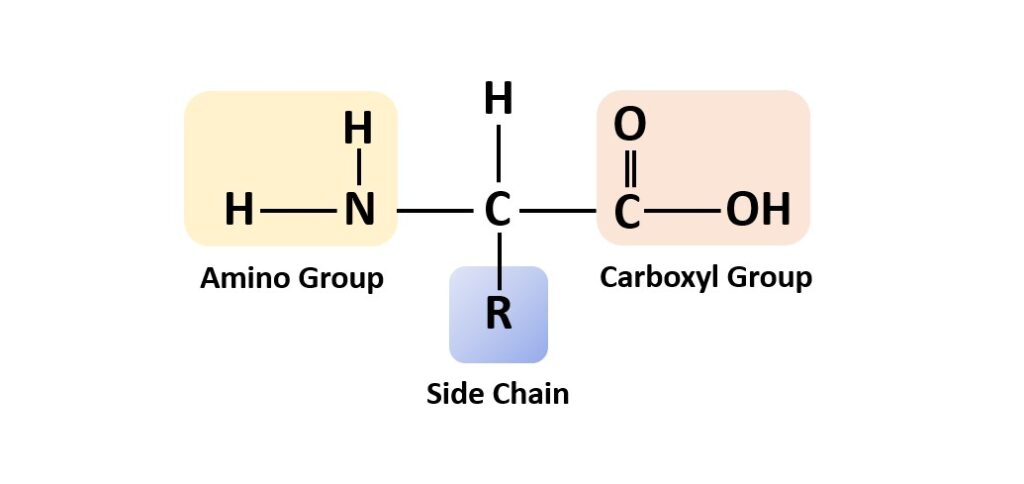
Fig. 1. Formula of an amino acid, which is the functional unit that comprises proteins.
Proteins participate in most functions of the organism including the transport of molecules, metabolic reactions, the synthesis and replication of DNA, and the response to stimuli (7). The different amino acid sequence characterizes the different proteins that fold and take on a specific structure which can be primary (the chain sequence of amino acids), secondary (a-helix shape), tertiary (three-dimensional unit of polypeptides), or quaternary (complex structure of polypeptide subunits). Fibrous structural proteins make up muscles, bones, and skin, defending the body from external insults, while globular proteins participate in cellular physiological functions and include enzymes, hormones, and antibodies.
Proper nutrition that is characterized by the correct consumption of nutrients in sufficient amounts, is the basis for maintaining the health of the body. Almost every food of animal or plant origin contains protein. However, the amino acid composition and the amount of protein varies amongst different foods (8). The highest levels of protein can be found in lean meats, fish, and legumes (9) (Table I).
Table I. List of the main foods containing high levels of protein.
| · Lean meats such as beef, chicken, turkey and lamb. |
| · Fish such as tuna, salmon, cod, sardines, mackerel and mussels. |
| · Legumes such as lentils, chickpeas, beans, peas, edamame and soy. |
Essential amino acids are those which cannot be synthesized by metabolic intermediates in the human body, and therefore must be introduced into the body externally by diet. Proteins are very important in the diet because they participate in the development of immune defenses, the growth and renewal of tissues, allow digestion, and are fundamental for the transport of oxygen in the blood (10). Protein deficiency causes an energy deficit with fatigue and difficulty concentrating and learning, amongst other problems (8) (Table II).
Table II. Some common dysfunctions related to protein deficiency.
| · reduced metabolic efficiency | · reduction in muscle volume |
| · alterations in sleep and digestion | · hair loss |
| · accumulation of stress and anxiety | · bad mood |
| · fluctuations in body weight | · muscle soreness |
| · swollen ankles and feet | · ease of bleeding |
| · dry and irritated skin with symptoms of premature aging (appearance of wrinkles) | · slow healing of wounds |
| · articular pains |
In subjects affected by cancer, there is an alteration of the metabolism and progressive weight loss, with damage to organs and tissues and a decrease in energy (11). Anti-cancer therapies often do not improve the patient’s weight recovery. Protein deficiency can lead to cachexia with loss of muscle tissue and nausea and vomiting (12), which can be aggravated by cancer therapies such as chemotherapy and radiotherapy (13).
Low protein plasma concentrations have been found in many disorders, including cancer (14). Tissue protein depletion appears to be common in patients with advanced cancer who have a loss of hepatic functions, including the ability to synthesize proteins (15). Therefore, administration of an oral supply of protein needs to and seems to be very effective in cancer patients. Ensuring nutritional requirements of protein in cancer patients is crucial to prevent and minimize negative health effects (16). The optimal intake of proteins and vitamins in cancer therapy can be of great help for the health and quality of life for patients.
In cancer patients with and without metastases, weight loss resulting as a consequence of low appetite must be counteracted. For this reason, the patient should consume foods with a high protein content. An effective therapy can include protein cocktails extracted from various foods such as meat, eggs, legumes, fish, and dried fruit, which is enriched with a set of multivitamins.
CONCLUSIONS
Therefore, we can conclude that in cancer patients and other pathologies that involve protein deficiency, the intake of protein from foods in combination with a high concentration protein supplement can be of great help in improving health and quality of life. A high-protein compound that contains essential amino acids and is free of fat and sodium could be indicated to compensate for protein deficiency.
Conflict of interest
The author declares that they have no conflict of interest.
REFERENCES
- Rivadeneira DE, Evoy D, Fahey TJ, Lieberman MD, Daly JM. Nutritional support of the cancer patient. CA: A Cancer Journal for Clinicians. 1998;48(2):69-80. doi:https://doi.org/10.3322/canjclin.48.2.69
- Setnick J. Micronutrient Deficiencies and Supplementation in Anorexia and Bulimia Nervosa. Nutrition in Clinical Practice. 2010;25(2):137-142. doi:https://doi.org/10.1177/0884533610361478
- Ensari A. The Malabsorption Syndrome and Its Causes and Consequences. Pathobiology of Human Disease. Published online 2014:1266-1287. doi:https://doi.org/10.1016/B978-0-12-386456-7.03804-1
- Lecker SH, Goldberg AL, Mitch WE. Protein Degradation by the Ubiquitin–Proteasome Pathway in Normal and Disease States. Journal of the American Society of Nephrology. 2006;17(7):1807-1819. doi:https://doi.org/10.1681/asn.2006010083
- Lanpher BC, Gropman A, Chapman KA, Lichter-Konecki U. Urea Cycle Disorders C, Summar ML: Urea cycle disorders overview. In GeneReviews. Edited by: Pagon RA, Bird TD, Dolan CR, Stephens K, Adam MP. Seattle: NCBI1993; Updated September 1,2011
- Rao M, Sharma M, Juneja R, Jacob S, Jacob CK. Calculated nitrogen balance in hemodialysis patients: Influence of protein intake. Kidney International. 2000;58(1):336-345. doi:https://doi.org/10.1046/j.1523-1755.2000.00171.x
- Alberts B, Johnson A, Lewis J. Molecular Biology of the Cell. 4th ed. Garland Science; 2002. Protein Function. Available from: https://www.ncbi.nlm.nih.gov/books/NBK26911/
- Wu G. Dietary Protein Intake and Human Health. Food & Function. 2016;7(3):1251-1265. doi:https://doi.org/10.1039/c5fo01530h
- van Vliet S, Burd NA, van Loon LJ. The Skeletal Muscle Anabolic Response to Plant- versus Animal-Based Protein Consumption. The Journal of Nutrition. 2015;145(9):1981-1991. doi:https://doi.org/10.3945/jn.114.204305
- Koithan M, Devika J. New Approaches to Nutritional Therapy. The Journal for Nurse Practitioners. 2010;6(10):805-806. doi:https://doi.org/10.1016/j.nurpra.2010.07.001
- Petruzzelli M, Wagner EF. Mechanisms of metabolic dysfunction in cancer-associated cachexia. Genes & Development. 2016;30(5):489-501. doi:https://doi.org/10.1101/gad.276733.115
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. The Lancet Oncology. 2011;12(5):489-495. doi:https://doi.org/10.1016/S1470-2045(10)70218-7
- Dodson S, Baracos VE, Jatoi A, et al. Muscle Wasting in Cancer Cachexia: Clinical Implications, Diagnosis, and Emerging Treatment Strategies. Annual Review of Medicine. 2011;62(1):265-279. doi:https://doi.org/10.1146/annurev-med-061509-131248
- Roberts JA, Pea F, Lipman J. The Clinical Relevance of Plasma Protein Binding Changes. Clinical Pharmacokinetics. 2012;52(1):1-8. doi:https://doi.org/10.1007/s40262-012-0018-5
- Tisdale MJ. Biology of cachexia. Journal of the National Cancer Institute. 1997;89(23):1763-1773. doi:https://doi.org/10.1093/jnci/89.23.1763
- Rand WM, Pellett PL, Young VR. Meta-analysis of nitrogen balance studies for estimating protein requirements in healthy adults. The American Journal of Clinical Nutrition. 2003;77(1):109-127. doi:https://doi.org/10.1093/ajcn/77.1.109